Bariatric Medication Absorption Calculator
Medication Absorption Calculator
Enter your surgery type and medication details to see how absorption may be affected.
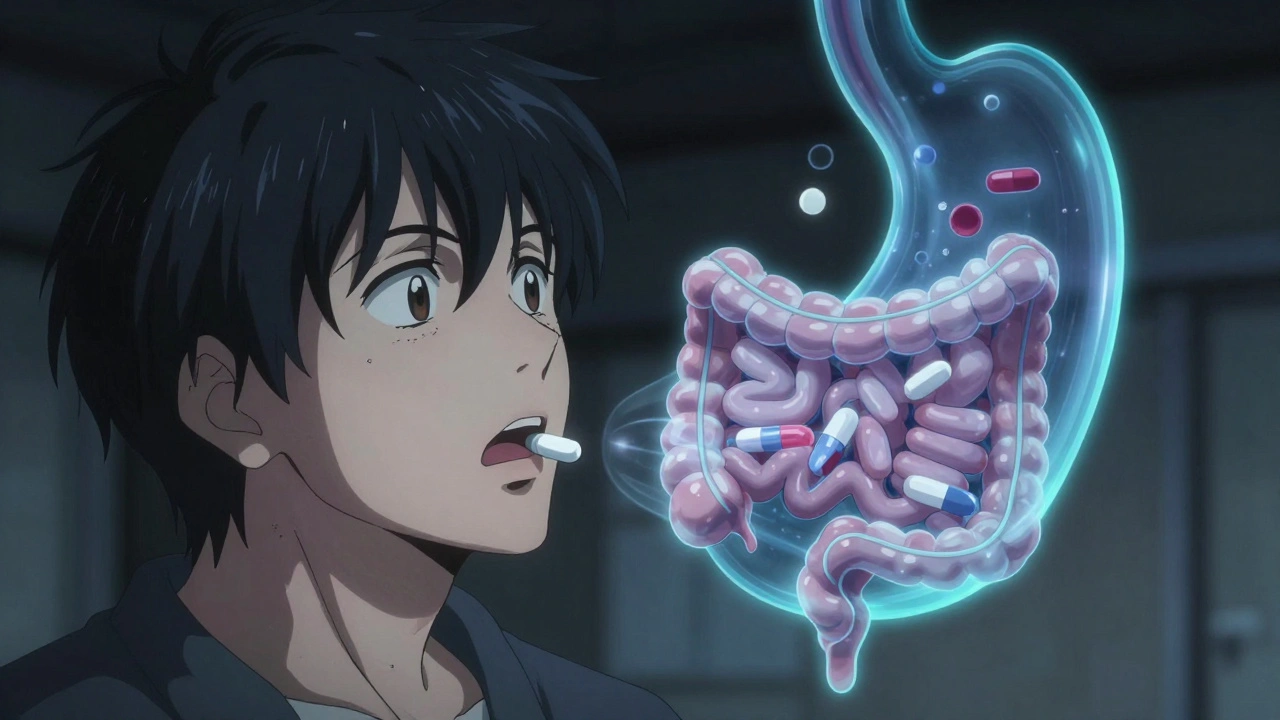
After bariatric surgery, many patients notice something strange: their medications don’t seem to work like they used to. A pill that once kept their blood pressure steady now feels useless. Their thyroid medication doesn’t control symptoms anymore. Painkillers that used to last eight hours are gone in two. This isn’t in their head. It’s physics, chemistry, and anatomy changing under the skin.
Why Your Pills Don’t Work Like They Used To
Bariatric surgery isn’t just about shrinking your stomach. It rewires your digestive system. In a Roux-en-Y gastric bypass (RYGB), doctors cut your stomach into a small pouch and reconnect the small intestine so food skips the first 100-150 cm of it. That’s about a quarter of your entire small intestine - the main place where most drugs get absorbed. In a sleeve gastrectomy, your stomach is reduced to the size of a banana, but the intestine stays mostly untouched. Even then, the acid level in your stomach rises from 1.5-3.5 pH to 4.0-6.0. That’s like switching from vinegar to weak lemonade.Drugs need the right environment to dissolve and get into your bloodstream. Acid-dependent drugs - like ketoconazole, itraconazole, or even levothyroxine - need low pH to break down. When your stomach becomes less acidic, these pills just sit there, undissolved. Extended-release tablets are designed to slowly release medicine over hours as they travel through your gut. But if your food and pills zip through the intestine in 30 minutes instead of 4 hours, the drug doesn’t have time to release properly. The result? Half the dose, or less, gets absorbed.
Procedure Matters: RYGB vs. Sleeve vs. BPD-DS
Not all surgeries are created equal when it comes to drug absorption. The type of surgery you had changes everything.- Roux-en-Y Gastric Bypass (RYGB): This is the most disruptive. About 68% of patients need medication changes. Drugs like metformin ER, glipizide XL, and oxycodone CR lose 30-60% of their effectiveness. Levothyroxine absorption drops by 25-30%. Warfarin levels become unpredictable - 60% of patients need higher doses.
- Sleeve Gastrectomy: Less dramatic. About 32% of patients need adjustments. The main issue is reduced stomach volume and higher pH. Tablets may not dissolve well. Liquid forms or crushed pills (if safe) work better. Bioavailability for most drugs drops only 15-20%.
- Biliopancreatic Diversion with Duodenal Switch (BPD-DS): The most extreme. Up to 70% of drugs are poorly absorbed. This procedure bypasses most of the small intestine. Patients often need 2-3 times the normal dose of vitamins, calcium, and some antidepressants.
- Gastric Banding: Minimal direct effect on absorption. But because you eat so little, food-dependent drugs like mycophenolate can become ineffective unless taken with a full meal.
Key takeaway: If your duodenum (the first part of your small intestine) is bypassed, expect major changes. If it’s still in the path, your risks are much lower.
Drugs That Always Need a Second Look
Some medications are notorious for failing after bariatric surgery. Here are the top offenders:- Levothyroxine: Thyroid hormone replacement. Absorption drops sharply after RYGB. Many patients go from 75mcg to 125mcg or higher. Take it on an empty stomach, 30-60 minutes before breakfast.
- Metformin ER: Extended-release diabetes drug. Often fails after RYGB. Switch to immediate-release metformin, taken 2-3 times daily. Dose may need to increase by 20-30%.
- Warfarin: Blood thinner. Levels swing wildly. One patient might need a 25% increase, another a 50% increase. Weekly INR checks for the first 3 months are non-negotiable.
- Extended-release opioids (oxycodone CR, morphine ER): Lose 40-60% efficacy. Switch to immediate-release versions. Don’t crush pills unless approved - some have abuse-deterrent coatings.
- Calcium and Vitamin D: Calcium carbonate needs stomach acid to dissolve. Switch to calcium citrate. Take 500-600mg doses 2-3 times daily. Vitamin D often requires 2,000-5,000 IU daily.
- Enteric-coated pills (aspirin EC, omeprazole): Designed to dissolve in the small intestine. If the duodenum is bypassed, they may pass through untouched. Switch to liquid or non-coated versions.
- Antiepileptics (phenytoin, carbamazepine): Narrow therapeutic window. Even small drops in absorption can trigger seizures. Therapeutic drug monitoring is essential.
- Immunosuppressants (cyclosporine, tacrolimus): Used after organ transplants. Levels can crash. Weekly blood tests are standard for the first 6 months.
What to Do: Practical Steps for Patients and Providers
If you’ve had bariatric surgery and are on meds, here’s what to do - now.- Don’t wait for symptoms. Schedule a medication review with a pharmacist or specialist within 30 days after surgery.
- Switch extended-release to immediate-release. If your drug is on the list above, ask if it can be changed. For example: metformin ER → metformin IR; glipizide XL → glipizide IR.
- Use liquids or crushable forms. For the first 3 months, liquid medications are safest. If you must take pills, ask if they can be crushed or opened (not all can - check with your pharmacist).
- Time your doses. Take acid-dependent drugs (thyroid, antifungals) 30-60 minutes before meals. Take fat-soluble drugs (some antidepressants, vitamins A/D/E/K) with meals.
- Monitor your levels. For warfarin, antiepileptics, immunosuppressants, and thyroid meds - regular blood tests are not optional. Track your INR, TSH, drug trough levels.
- Report failures immediately. If your pain returns, your mood drops, your blood sugar spikes, or you feel dizzy - don’t assume it’s just recovery. It could be your meds.
One patient in Manchester told his pharmacist he was ‘taking his thyroid pill like always’ - but after RYGB, he was swallowing it with coffee right after breakfast. That’s the worst possible way. He switched to taking it with water at 6 a.m., before any food or drink. His TSH normalized in 4 weeks.
The New Standard of Care
The American Society for Metabolic and Bariatric Surgery (ASMBS) now recommends preoperative medication planning. That means before surgery, your doctor and pharmacist should sit down and review every pill you take. They should map out which ones need switching, which ones need dose increases, and which ones are safe to leave alone.Pharmacies in the UK and US are starting to hire specialists just for bariatric patients. The American Society of Health-System Pharmacists reports a 200% increase in these roles since 2018. Hospitals now use 5-step assessment tools to reduce medication errors by over a third. AI-powered dosing calculators are being rolled out in 83 US hospitals - they factor in your surgery type, weight, and drug profile to suggest exact doses.
The FDA and EMA have started requiring drug manufacturers to test how their products behave after bariatric surgery. Eight extended-release drugs now carry warnings on their labels. That’s progress.
What’s Next: Better Pills for a Changed Body
Science is catching up. Researchers at the University of Copenhagen are testing pH-adaptive capsules that dissolve even in high-pH environments. These could make levothyroxine and other acid-dependent drugs work again without changing the dose.Intarcia’s ITCA 650 - a tiny implant that slowly releases exenatide under the skin - bypasses the gut entirely. In RYGB patients, it worked 92% of the time. Oral versions only worked 68%. That’s the future: avoid the gut if the gut can’t be trusted.
And in the next 5 years, pharmacogenomics may become routine. Your DNA could tell your doctor if you’re a fast or slow metabolizer of certain drugs. Combine that with your surgical anatomy, and dosing becomes personalized - not guesswork.
For now, the rule is simple: if you’ve had bariatric surgery, assume your meds have changed. Don’t wait for something to go wrong. Talk to your pharmacist. Get your levels checked. Switch formulations early. Your health depends on it.
Do all bariatric surgeries affect medication absorption the same way?
No. RYGB and BPD-DS cause major changes because they bypass parts of the small intestine. Sleeve gastrectomy mainly affects stomach acidity and volume, so changes are milder. Gastric banding has little direct impact. The key question is: Was your duodenum bypassed? If yes, expect significant absorption changes.
Can I still take my extended-release pills after surgery?
Usually not. Extended-release tablets are designed to release medicine slowly over hours as they move through your intestines. After RYGB or BPD-DS, pills zip through too fast - they don’t have time to release properly. Most patients need to switch to immediate-release versions. Always check with your pharmacist before making changes.
Why does my thyroid medication not work anymore after gastric bypass?
Levothyroxine needs an acidic environment to dissolve. After RYGB, your stomach pH rises from 1.5-3.5 to 4.0-6.0, making it harder for the pill to break down. Also, the part of the intestine where it’s absorbed may be bypassed. Most patients need a 25-50% dose increase and must take it on an empty stomach, 30-60 minutes before food.
Should I crush my pills after bariatric surgery?
Only if your pharmacist says it’s safe. Some pills have special coatings - extended-release, enteric-coated, or abuse-deterrent - that are ruined if crushed. Others, like generic metformin or some antidepressants, can be safely crushed or opened. Never assume. Always ask.
How long after surgery do medication changes take effect?
Changes can happen within days to weeks. For drugs like warfarin or levothyroxine, effects may show up in 1-2 weeks. For others, like antidepressants, it might take 4-6 weeks to notice a difference. That’s why follow-up blood tests are critical in the first 3-6 months.
Is it safe to take vitamins with my medications?
Some vitamins interfere with drugs. Calcium and iron can block absorption of antibiotics, thyroid meds, and bisphosphonates. Take them at least 4 hours apart. Use calcium citrate, not carbonate - it’s better absorbed in low-acid environments. Always space out your meds and vitamins unless told otherwise.
What should I do if I can’t afford to switch to brand-name immediate-release drugs?
Generic immediate-release versions are widely available and much cheaper. For example, generic metformin IR costs less than $5 a month. Ask your pharmacist to compare prices. Many pharmacies offer discount programs. Don’t skip doses because of cost - there are affordable options.
Can I go back to my old dose if I feel fine?
No. Feeling fine doesn’t mean your drug levels are right. For drugs like warfarin or antiepileptics, even small drops in absorption can lead to serious problems - blood clots or seizures. Always follow lab results, not how you feel.

Write a comment
Your email address will not be published.
Recent Posts
-
 Recent Patent Cases and Generic Delays: 2023-2025 Examples December 19, 2025
Recent Patent Cases and Generic Delays: 2023-2025 Examples December 19, 2025 -
 Anhydrous Crystalline Maltose: Boost Energy & Stamina in Your Diet September 22, 2025
Anhydrous Crystalline Maltose: Boost Energy & Stamina in Your Diet September 22, 2025 -
 Nitrofurantoin and Fertility: What You Should Know October 28, 2025
Nitrofurantoin and Fertility: What You Should Know October 28, 2025


9 Comments
omg i literally just had gastric bypass last year and thought i was going crazy bc my thyroid meds weren't working 😭 i was taking them with coffee like a dummy... switched to water at 6am and my tsh normalized in like 3 weeks. thank you for this post, i feel less alone 💕
The physiological dislocation of pharmacokinetic pathways post-RYGB represents a paradigm shift in bioavailability determinants. The duodenal bypass fundamentally alters the pH-dependent dissolution kinetics of weakly basic compounds, while simultaneously shortening transit time-thereby compromising the sustained-release mechanisms of ER formulations. This is not merely a dosing issue; it's a pharmacodynamic reconfiguration of the host-environment interface.
my dr never told me any of this and i almost had a seizure from my epilepsy med dropping too low… i’m so glad i found this. pls tell everyone you know. this could save lives 💪❤️
There’s a deeper ethical layer here: if pharmaceutical companies aren’t required to test drugs in post-bariatric populations, are we treating patients or just optimizing for clinical trial compliance? The FDA’s recent label updates are a start, but systemic change requires rethinking how we define ‘standard dosing’ altogether.
lol so you're telling me the government and big pharma don't want you to know that surgery makes your pills useless? they're just letting you take the same dose and then blaming you when you get sick... next they'll say your stomach is 'not cooperating' 😏
so basically your body just stops working after surgery? how is this even legal? why aren't these people suing?
THIS IS SO IMPORTANT. I’m a nurse and I’ve seen too many patients come in confused and scared because their meds stopped working. Please, if you’re post-op, go see a pharmacist. They’re the real heroes here. And if you’re a provider-don’t assume your patient knows this stuff. Educate them like their life depends on it. Because it does. 💙
Interesting that you mention AI-powered dosing calculators, but you completely ignore the fact that most of these algorithms are trained on non-bariatric populations. The so-called 'progress' is just statistical band-aiding. Real innovation would require re-engineering drug delivery systems from the ground up-not slapping a patch on broken pharmacokinetic models.
Let me be clear: if your doctor didn’t discuss medication changes before or after your surgery, they’re not doing their job. This isn’t optional. It’s standard of care. You are not being dramatic. You are not overreacting. You are being medically neglected. Go back. Bring this article. Demand a pharmacist consult. Your life is not a guessing game.