
When a pharmacist hands you a pill bottle with a different name than what your doctor wrote, you might wonder: Is this really the same drug? It’s not just branding. It’s science, law, and a strict set of standards that ensure you get the same effect-without paying more.
The Science Behind Generic Substitution
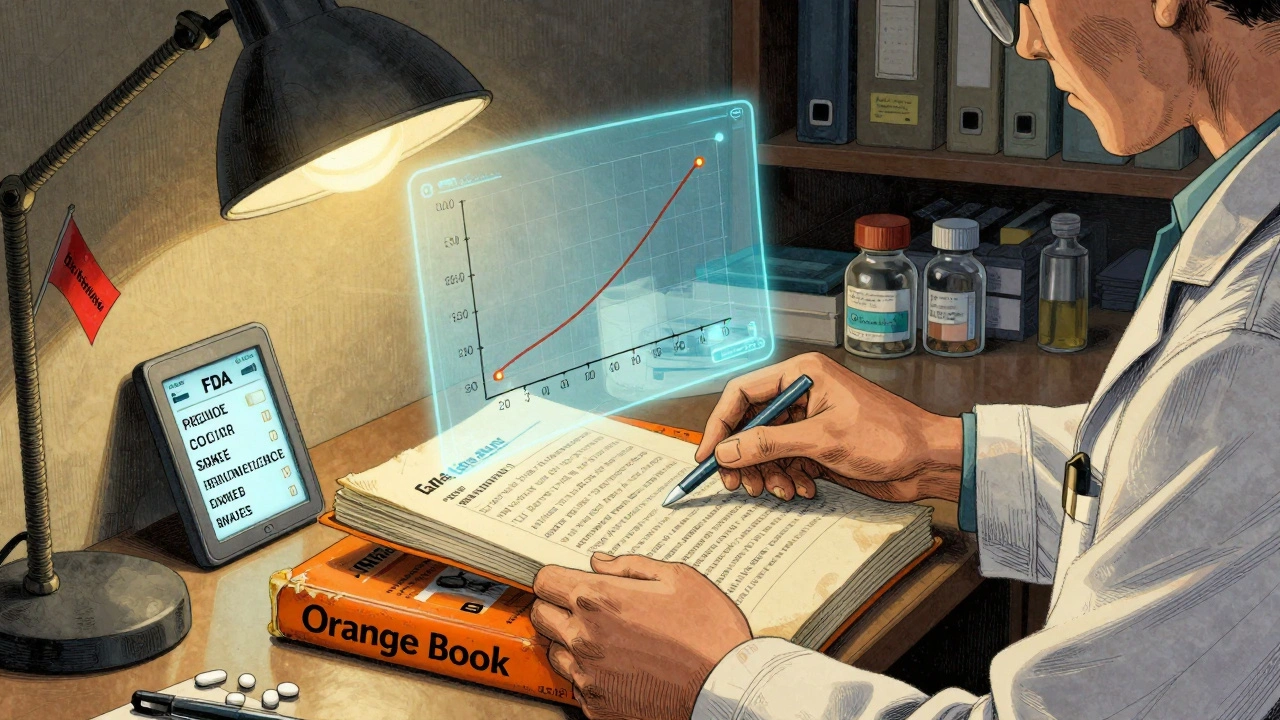
Generic drugs aren’t copies. They’re exact replicas in active ingredients, strength, dosage form, and how they’re taken. But that’s only the start. The real question is: do they work the same way in your body? That’s where bioequivalence comes in. Before a generic drug can be approved, the manufacturer must prove it releases the same amount of active ingredient into your bloodstream at the same rate as the brand-name version. The FDA requires the 90% confidence interval for two key measurements-maximum concentration (Cmax) and total exposure (AUC)-to fall between 80% and 125%. This isn’t a guess. It’s based on decades of clinical data showing that within this range, there’s no meaningful difference in how the drug works. For most drugs, this works perfectly. But for drugs with a narrow therapeutic index-like warfarin, levothyroxine, or phenytoin-the window tightens to 90-111%. Even a small shift can cause serious side effects or make the drug ineffective. That’s why pharmacists pay extra attention to these.The Orange Book: The Pharmacist’s Legal Bible
The U.S. Food and Drug Administration’s Approved Drug Products with Therapeutic Equivalence Evaluations-better known as the Orange Book-is the single most important tool a pharmacist uses to verify generic equivalence. First published in 1980, it’s updated monthly and contains over 16,500 drug products as of April 2024. Each entry has a two-letter code that tells pharmacists whether substitution is safe:- AB: Therapeutically equivalent. This is the gold standard. Over 98.7% of rated products fall into this category.
- A: Pharmaceutically equivalent but lacks bioequivalence data (rare).
- B: Not considered equivalent. Never substitute.
- AN, AO, AT: Special codes for complex forms like nasal sprays, oral solutions, or topical creams.
How Pharmacists Verify Equivalence in Practice
It’s not complicated, but it’s methodical. Here’s the step-by-step process most pharmacists follow:- Identify the reference drug-the original brand-name product listed in the prescription.
- Match the active ingredient, strength, and dosage form-if the generic doesn’t match exactly, it’s not interchangeable.
- Check the Orange Book’s TE code-only products with an 'A' rating (usually AB) are approved for substitution.
- Confirm no ‘Do Not Substitute’ flag-if the prescriber wrote ‘dispense as written’ or ‘brand necessary,’ substitution is illegal, regardless of the rating.
What Happens When a Drug Isn’t in the Orange Book?
About 5.7% of generic substitutions involve drugs not yet listed. This happens with newer products or complex formulations like inhalers, transdermal patches, or compounded generics. In these cases, pharmacists can’t rely on the Orange Book alone. They turn to other trusted resources: Micromedex, Lexicomp, or First Databank. But here’s the key-they don’t substitute unless they have clear, documented evidence of equivalence. The FDA provides guidance for these situations, called the Non-Orange Book Listed Drugs framework. It requires pharmacists to document their reasoning, consult with the prescriber if needed, and ensure the product meets FDA standards for manufacturing and testing. In 2019, a pharmacist in Texas was sanctioned after substituting a non-Orange Book product without proper documentation. The court ruled: “Relying on commercial databases alone is not sufficient.” The Orange Book is the law. Everything else is backup.Why This System Works-And Where It’s Still Evolving
The system isn’t perfect, but it’s proven. A 2020 FDA meta-analysis of over 1 million patient records found no statistically significant difference in adverse events between brand and generic drugs-0.78% vs. 0.81%. That’s less than one extra adverse event per 10,000 prescriptions. But challenges remain. Complex products like inhalers or topical corticosteroids don’t always behave the same way in the body even if blood levels match. Dr. Randall Stafford from Stanford pointed out in JAMA Internal Medicine that traditional bioequivalence metrics may miss real-world differences in how these drugs are absorbed through skin or lungs. That’s why the FDA has developed over 1,850 product-specific guidances since 2020. These give manufacturers detailed requirements for testing complex generics. The agency also allocated $28.5 million through GDUFA III in 2023 to improve bioequivalence methods for these drugs. Biosimilars-biologic generics-are the next frontier. Unlike small-molecule generics, they’re made from living cells. As of June 2024, only 47 of 350 approved biosimilars are listed in the FDA’s Purple Book, the biologics equivalent of the Orange Book. Pharmacists are still learning how to verify these. Training programs are expanding, but the system isn’t fully ready.
The Bigger Picture: Why This Matters
Generic drugs now make up 90.7% of all prescriptions filled in the U.S.-over 8.9 billion in 2023. That’s a $12.7 billion annual savings for patients and the health system. But none of that matters if the substitution isn’t safe. Pharmacists are the final checkpoint. They don’t just count pills. They verify science, interpret law, and protect patients. Every time they check the Orange Book, they’re not just following procedure-they’re ensuring a patient gets the same treatment they were prescribed, at a price they can afford. Training is strict. Ninety-two percent of pharmacies require new hires to complete 2-4 hours of Orange Book training. Competency tests show 89.3% accuracy after training. That’s not luck. That’s discipline. And as more complex drugs enter the market, the role of the pharmacist isn’t shrinking-it’s growing. The system works because it’s grounded in data, enforced by law, and upheld by professionals who know exactly what they’re doing.Can a pharmacist substitute a generic drug without the prescriber’s permission?
Yes, but only if three conditions are met: the generic is rated ‘A’ in the FDA Orange Book, the prescription doesn’t say ‘dispense as written,’ and state law permits substitution. Forty-nine states allow automatic substitution under these rules. Massachusetts is the exception-it requires prescriber consent for all substitutions.
Are all generic drugs in the Orange Book?
No. About 5.7% of generic drugs aren’t listed yet, especially newer products or complex formulations like inhalers or topical creams. Pharmacists must use additional resources and professional judgment in these cases, but they cannot substitute unless they have clear evidence of equivalence from FDA-approved studies.
What does an ‘AB’ rating mean in the Orange Book?
An ‘AB’ rating means the generic drug is both pharmaceutically equivalent (same active ingredient, strength, dosage form) and bioequivalent (proven to work the same way in the body) to the brand-name drug. It’s the only rating that allows legal substitution in all 50 U.S. states.
Why do some generics have different shapes or colors than the brand name?
The active ingredient must be identical, but inactive ingredients-like fillers, dyes, or coatings-can differ. These affect appearance, taste, or how quickly the pill dissolves, but not how the drug works. The FDA allows these differences as long as bioequivalence is proven. A pill’s color or shape has no impact on its effectiveness.
Is there a risk of side effects when switching from brand to generic?
For most people, no. FDA data shows adverse event rates are statistically identical between brand and generic drugs. Rare exceptions occur with narrow therapeutic index drugs, where even tiny differences matter. In those cases, pharmacists use tighter bioequivalence standards and may consult with the prescriber before switching.
How often is the Orange Book updated?
The FDA updates the Orange Book monthly with supplements and releases a full annual edition. Pharmacists are trained to check for the latest updates, especially when a new generic enters the market. Outdated information can lead to incorrect substitution decisions.
Can pharmacists use other databases instead of the Orange Book?
They can use other databases like Micromedex or Lexicomp as secondary tools, but the Orange Book is the only legally recognized standard for substitution decisions. Relying solely on commercial databases has led to disciplinary actions. The Orange Book is the law, not a suggestion.
What happens if a pharmacist substitutes incorrectly?
If a pharmacist substitutes a drug not rated ‘A’ in the Orange Book-or ignores a ‘do not substitute’ order-they can face disciplinary action from the state board of pharmacy, malpractice claims, or even license suspension. In the 2019 Texas case State Board of Pharmacy v. Smith, a pharmacist was sanctioned for substituting a non-Orange Book-listed product without proper documentation.
Next Steps for Pharmacists
If you’re a pharmacist, make sure you’re using the latest version of the Orange Book-check for monthly updates. If your pharmacy software doesn’t auto-update, subscribe to the FDA’s email alerts. Train new staff every year, not just during onboarding. And always document your decisions, especially for non-listed drugs. If you’re a patient and you’re unsure about a generic substitution, ask your pharmacist: “Is this approved by the FDA as equivalent?” They’re trained to explain it clearly. You don’t need to know the science-but they do, and they’re there to make sure you’re safe.
Write a comment
Your email address will not be published.
Recent Posts
-
 Buy Cheap Generic Celebrex Online - Safe Guide & Best Prices September 28, 2025
Buy Cheap Generic Celebrex Online - Safe Guide & Best Prices September 28, 2025




8 Comments
so i got my generic adderall last week and was like... wait, this pill looks nothing like the blue one? then i checked the bottle and saw AB rating and was like ok cool, pharmacists are wizards 🤓
yo if you don’t know what Cmax and AUC stand for you’re literally putting your life in the hands of someone who’s probably scrolling through tiktok during their break. bioequivalence isn’t a suggestion, it’s a 90% CI between 80-125%-that’s FDA math, not guesswork. and if your pharmacy uses some sketchy database instead of the Orange Book? bro, that’s how you end up in court. #pharmacistlife
okay but let’s be real-what about the people who switch from brand to generic and suddenly feel like a zombie? i know a guy who went from brand Lipitor to generic and started having muscle cramps so bad he couldn’t walk his dog. he went back to brand and boom-fixed. so yeah, ‘statistically insignificant’ doesn’t mean ‘doesn’t happen.’ and don’t even get me started on levothyroxine. one milligram off and you’re either dead or on a treadmill at 3am sweating through your shirt. this system works… until it doesn’t.
PHARMACISTS ARE UNSUNG HEROES 💪❤️🔥
they’re the ones checking the orange book while you’re scrolling on your phone
they’re the ones catching errors before you swallow something dangerous
they’re the ones explaining why your pill is pink now and not blue
they’re the ones making sure you don’t pay $300 for a pill that costs $3
thank you, pharmacy team 🙌👏👏👏
the fact that people still think generics are ‘inferior’ is wild. we’re talking about the same active ingredient, same bioavailability, same FDA scrutiny. if you’re worried about color or shape, go buy a crayon. the science is locked in. and if your pharmacist doesn’t use the orange book? fire them. simple as that. no drama, no ‘but my cousin said…’-just facts. 🚫💊❌
oh wow, another article about how pharmacists are basically saints who never make mistakes. funny how the same people who scream ‘big pharma is evil!’ are fine with generics that cost 90% less. but hey, if the FDA says it’s safe, i guess we all just trust the algorithm, right? 🙄
also, ‘99.3% of pharmacists rely on it’-cool. what about the 0.7% who got fired for substituting without checking? you think they were all just lazy? or maybe the system’s got cracks you’re pretending aren’t there?
As someone who works in a community pharmacy in Ontario, I can confirm that while Canada doesn’t use the Orange Book, our equivalent-the Drug Product Database-is held to similar standards. The principles of bioequivalence, therapeutic equivalence, and documentation are universal. What’s remarkable is how consistently pharmacists across jurisdictions uphold these standards, even when under time pressure. It’s not just about compliance-it’s about ethical responsibility. Kudos to the U.S. system for its rigor.
@5800 yeah but canada’s system doesn’t have 50 different state laws. here, if you’re in Texas and the prescriber wrote ‘dispense as written’ but your software auto-subbed because it’s AB-rated? boom-you’re liable. we’re playing 4D chess with regulations while the FDA updates the orange book every month. no wonder some pharmacists just say ‘nah, i’ll just give the brand.’