
For 1 in 3 people with psoriasis, the skin condition isn't the only problem-they also develop painful joint damage that can change their lives forever. This isn't just a coincidence; it's psoriatic arthritis, a condition where the same immune system that attacks skin cells also targets joints.
What is Psoriatic Arthritis?
Psoriatic Arthritis is a chronic autoimmune disorder where the immune system attacks healthy skin and joint tissue, causing inflammation in both areas. It affects about 30% of people with psoriasis. Symptoms usually show up between ages 30 and 50, but it can happen at any age. In 15% of cases, joint pain appears before skin patches, making diagnosis harder.
Unlike regular arthritis, psoriatic arthritis is systemic. This means the immune system doesn't just target joints-it also attacks skin, nails, tendons, and even eyes. The connection between skin and joint issues is key. When your body overreacts to skin inflammation, it sends inflammatory signals to your joints, causing swelling and damage.
Common Symptoms
Psoriatic arthritis symptoms vary widely. Most people experience:
- Joint pain and stiffness, especially in the morning or after resting
- Swollen fingers or toes (called dactylitis or "sausage digits")
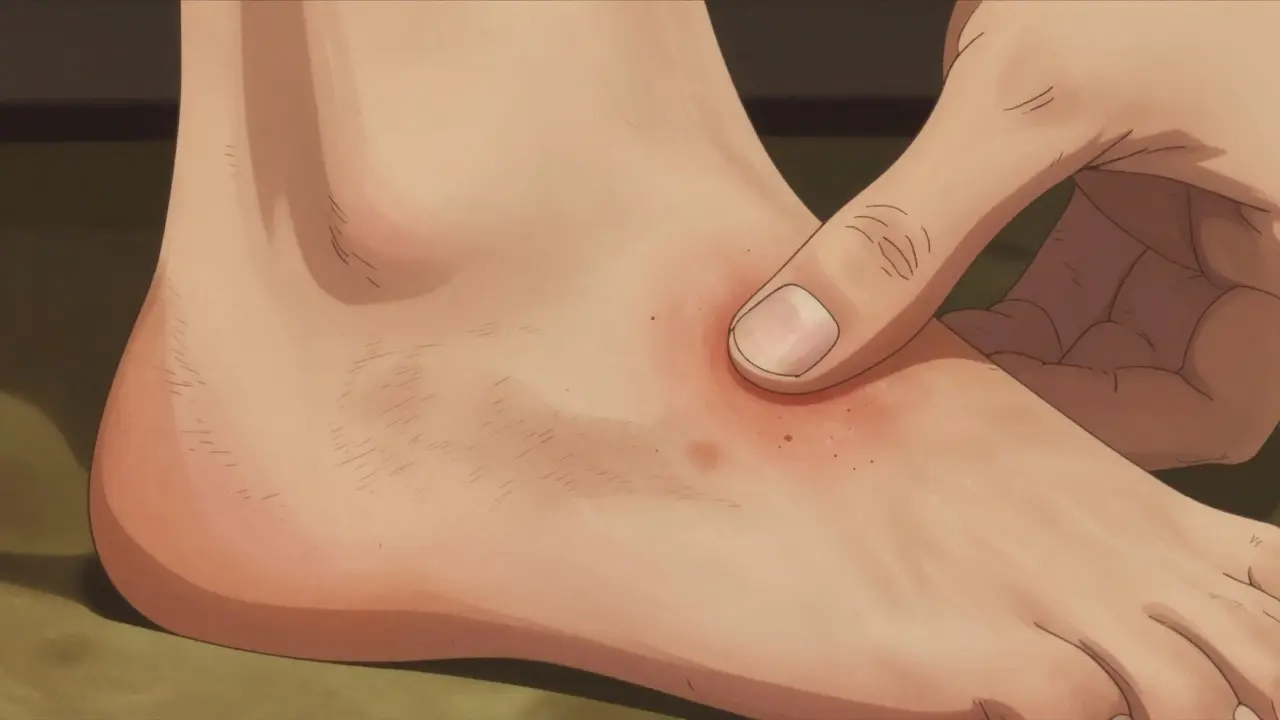
- Pain where tendons attach to bones (enthesitis), like in the Achilles tendon or bottom of the foot
- Nail changes like pits, discoloration, or separation from the nail bed
According to the Hopkins Arthritis Center, 92% of patients report morning stiffness lasting over 30 minutes. Dactylitis affects 40-50% of people with PsA, making fingers or toes look like sausages due to swelling in joints and tendons. Enthesitis occurs in 35-50% of cases, with the Achilles tendon and plantar fascia being common hotspots.
Five Types of Psoriatic Arthritis
Doctors classify PsA into five distinct types based on symptoms:
- Asymmetric oligoarthritis (35-40% of cases): Affects fewer than five joints unevenly, like the left knee but not the right
- Symmetric polyarthritis (25-30%): Similar joints on both sides, often mistaken for rheumatoid arthritis
- Distal interphalangeal predominant (DIP) (25%): Targets joints closest to nails, rarely seen in other arthritis types
- Spondylarthritis (5-10%): Causes spinal inflammation, leading to back pain that worsens with rest
- Arthritis mutilans (less than 5%): Severe bone loss causing "opera glass hand" deformities
Each type requires different management. For example, spondylarthritis often needs spinal-focused treatments, while DIP arthritis responds better to therapies targeting nail and joint inflammation.
Differences from Other Arthritis Types
| Feature | Psoriatic Arthritis | Rheumatoid Arthritis | Osteoarthritis |
|---|---|---|---|
| Joint pattern | Asymmetric (70% of cases) | Symmetric (90% of cases) | Variable, often weight-bearing joints |
| Rheumatoid factor | Negative | Positive in 80% | Negative |
| Nail changes | Common (80% of cases) | Rare | None |
| Bone changes | "Pencil-in-cup" deformities, new bone growth | Joint erosion | Bone spurs, cartilage loss |
This table shows why PsA is unique. Unlike rheumatoid arthritis (RA), which always affects both sides equally and tests positive for rheumatoid factor, PsA often hits joints unevenly and tests negative for that marker. Osteoarthritis (OA) is purely wear-and-tear damage without autoimmune involvement. PsA's nail changes and specific bone patterns on X-rays help doctors distinguish it from other conditions.
Why Early Diagnosis Matters
Delays in diagnosis cause permanent damage. The Toronto Psoriatic Arthritis Clinic found patients with delays over 12 months had 3.2 times more joint damage after five years. Many people wait years to get diagnosed-78% of survey respondents reported 2-5 years of delays.
One Reddit user shared: "I had 18 months of worsening joint pain before my rheumatologist connected my nail pitting to my skin patches. By then, three fingers were already damaged." Early signs like persistent joint stiffness, unexplained fatigue, or nail pitting should prompt a doctor visit. Dermatologists and rheumatologists working together catch PsA 82% of the time in integrated care models.

Treatment Options
Modern treatments stop joint damage before it starts. TNF inhibitors are biologic drugs that block tumor necrosis factor, reducing inflammation in psoriatic arthritis. They work for 45% of moderate-to-severe cases. For those who don't respond, IL-17 inhibitors target interleukin-17 pathways, with 72% of patients reporting significant pain relief within 12 weeks.
Common medications include:
- Methotrexate a conventional DMARD used in 65% of newly diagnosed patients
- TNF inhibitors like adalimumab or etanercept
- IL-17 inhibitors such as secukinumab or ixekizumab
Early intervention is key. Starting biologics within six months of symptoms reduces radiographic progression by 73% at two years. However, 30% of patients need to switch therapies after first-line treatment fails. Personalized treatment plans based on symptoms and biomarkers are becoming standard.
Living with Psoriatic Arthritis
PsA affects more than just joints. Sixty-five percent of patients experience moderate-to-severe fatigue that limits daily activities. Fifty-two percent face work disability within ten years. Common triggers include stress (85% of patients), infections (63%), and cold weather (57%).
But there's hope. A Psoriasis Foundation survey found 72% of patients on IL-17 inhibitors saw major pain improvement within three months. "My IL-17 inhibitor cut my joint pain in half," says one participant. "I can finally play with my kids again." Managing PsA means combining medication with lifestyle changes: weight control, stress reduction, and regular exercise.
What's Next for Psoriatic Arthritis?
Research is accelerating. The 2023 ACR/EULAR classification criteria now use imaging and biomarkers for 92% diagnostic accuracy. New drugs like guselkumab (an IL-23 inhibitor) achieved 64% symptom improvement in clinical trials. By 2027, doctors expect to use genetic tests to match patients with the best treatment, boosting efficacy by 40%.
Current studies focus on preventing PsA before it starts. The GO-ALIVE study shows early biologic therapy within six months of symptoms reduces joint damage by 73%. This shift toward proactive care could change outcomes for millions.
How is psoriatic arthritis diagnosed?
Doctors diagnose PsA through physical exams, imaging, and lab tests. They check for skin and nail psoriasis, joint swelling, and enthesitis pain. X-rays reveal unique bone changes like "pencil-in-cup" deformities. Blood tests rule out rheumatoid arthritis by testing negative for rheumatoid factor. Early diagnosis prevents permanent joint damage.
Can psoriasis cause joint pain?
Yes. Psoriatic arthritis develops when the immune system attacks both skin and joints. About 30% of people with psoriasis develop joint symptoms. Nail changes often appear before joint pain, serving as an early warning sign. If you have psoriasis and new joint discomfort, see a rheumatologist.
What's the difference between psoriatic arthritis and rheumatoid arthritis?
PsA and RA both cause joint inflammation, but they're different diseases. PsA often affects joints unevenly (like left knee but not right), tests negative for rheumatoid factor, and includes skin/nail changes. RA typically hits joints symmetrically, tests positive for rheumatoid factor, and rarely affects nails. X-rays show distinct bone patterns: PsA has "pencil-in-cup" deformities, while RA shows uniform joint erosion.
Is psoriatic arthritis hereditary?
Genetics play a role. If a close relative has psoriasis or PsA, your risk increases. Specific genes like HLA-B27 are linked to PsA, especially spinal involvement. But having the genes doesn't guarantee you'll develop it-environmental triggers like infections or stress often start the process. About 40% of PsA patients have family members with psoriasis or arthritis.
Can diet affect psoriatic arthritis?
Yes. Obesity increases PsA risk by 2.3-fold. Losing weight reduces inflammation and improves treatment response. Anti-inflammatory diets (rich in fish, vegetables, and whole grains) may help. Avoiding processed foods, sugar, and alcohol can cut flare-ups. While diet alone won't cure PsA, it supports medication effectiveness and overall health.

Write a comment
Your email address will not be published.




9 Comments
Hey I've been dealing with psoriatic arthritis for years and it's been tough but there are ways to manage it
Regular low impact exercise like swimming really helps with stiffness
Keeping a food journal helped me see that gluten makes my symptoms worse
Don't give up there's hope
I know it's frustrating but there are treatments that work
My rheumatologist was a lifesaver
The key is finding the right doctor and sticking with it
It's not easy but you can live a good life
Just take it one day at a time
You're not alone in this
As a medical professional I must say this article is misleading! Psoriatic arthritis isn't autoimmune it's just a symptom of poor lifestyle choices! Americans should focus on proper nutrition and exercise instead of relying on drugs! The real solution is in our own hands! The government is pushing unnecessary medications! We need to take responsibility for our health! Stop taking those expensive biologics! Just eat healthy and you'll be fine! It's all about personal responsibility! This is why America is the best country for healthcare!
Actually PsA is caused by 5G radiation! 😂
As someone who has studied this extensively I must say the mainstream medical community is completely wrong about psoriatic arthritis
The real cause isn't autoimmune but rather a result of 5G radiation and chemtrails
The government and pharmaceutical companies are hiding the truth to keep people dependent on expensive biologics
I've done my own research and found that a combination of ozone therapy and raw garlic can cure PsA completely
They don't want you to know this because it's not profitable
I've seen patients go from wheelchair-bound to fully functional within weeks using this method
The evidence is clear if you look beyond the propaganda
The FDA and WHO are in cahoots with Big Pharma
They suppress natural cures to maintain their profits
I'm not saying it's easy but if you're willing to do the research you can beat this
Don't trust the doctors they're all in on it
My cousin was cured after trying this and now he's living pain free
It's time to wake up and take control of your health
The studies they publish are all biased and funded by drug companies
You have to take matters into your own hands
Stop taking their medications and try natural remedies instead
Psoriatic arthritis can be challenging but there's hope. Early diagnosis and treatment make a huge difference. I recommend seeing a rheumatologist as soon as possible. Medications like TNF inhibitors and IL-17 blockers have helped many people. Also, lifestyle changes like weight management and stress reduction can support treatment. You're not alone-there's a community out there ready to help. Keep fighting!
I understand your perspective but the medical evidence clearly shows PsA is autoimmune. It's important to focus on treatments that work for patients. Maybe we can find a middle ground between lifestyle changes and medical care.
PsA is tough but we can handel it! Stay positive! 😊
I appreciate Carol's perspective but the medical consensus is clear. Let's work together on evidence-based treatments for PsA.
This is all wrong.