
When you pick up a prescription at the pharmacy, you might be handed a pill that looks completely different from the one you got last time. The name on the box isn’t the same. The color is off. Maybe it’s cheaper. And you wonder: is this really the same thing?
It is. And here’s why.
What Bioequivalence Testing Actually Measures
Bioequivalence testing isn’t about whether a generic drug works in theory. It’s about whether it works in your body - the same way the brand-name version does. The FDA defines it simply: if two drugs deliver the same amount of active ingredient at the same speed, they’re bioequivalent. That’s it.
The test looks at two numbers: AUC and Cmax. AUC stands for area under the curve - it tells you how much of the drug gets into your bloodstream over time. Cmax is the maximum concentration - how high the drug spikes in your blood after you take it. For a generic to be approved, its AUC and Cmax must fall within 80% to 125% of the brand-name drug’s values. That’s not a guess. It’s a scientifically proven range.
Think of it like this: if the brand drug gets you to 100 units of medicine in your blood, the generic has to get you between 80 and 125. Not 79. Not 126. That’s the rule. And every single generic approved in the U.S. has passed this test.
How the Test Is Done - And Who Takes Part
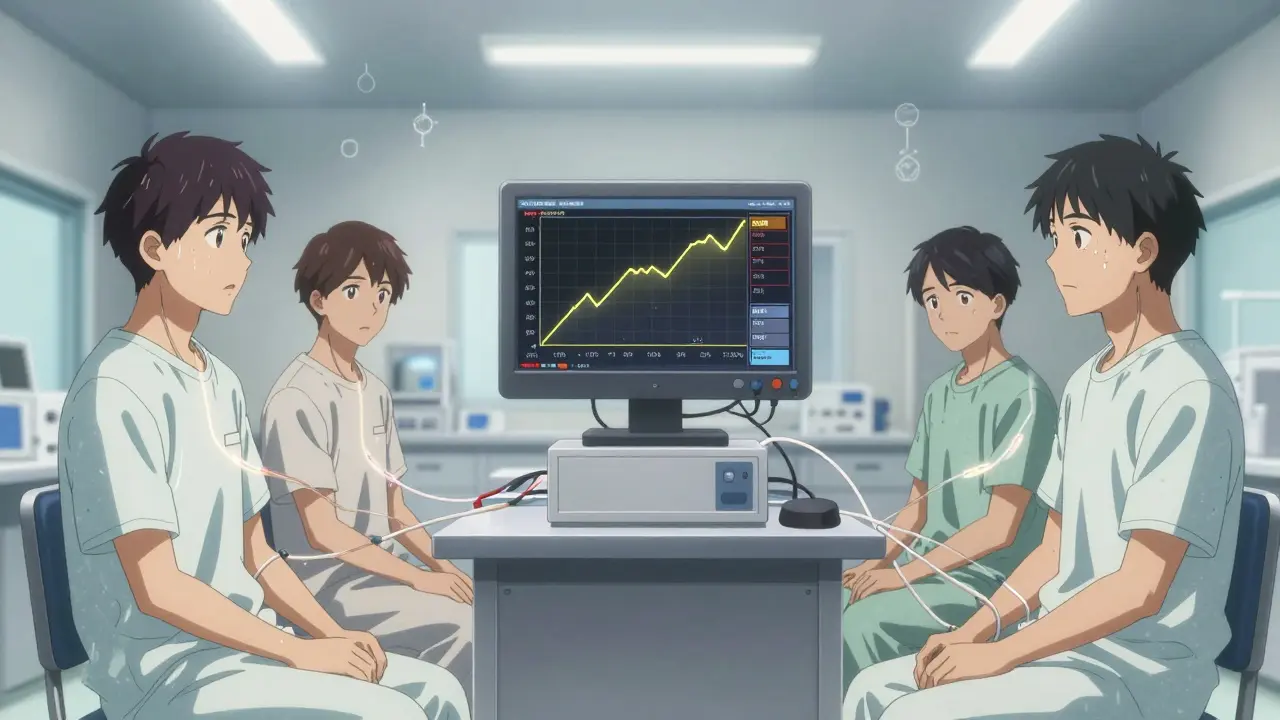
The study isn’t done on patients. It’s done on healthy volunteers - usually between 24 and 36 people. They come in, fast overnight, and take either the brand or the generic. Then they switch. This is called a crossover design. Blood samples are taken every 15 to 30 minutes for up to 24 hours. The data is plotted, analyzed, and compared.
Why healthy people? Because we’re not testing whether the drug cures cancer or lowers blood pressure. We’re testing whether it enters the bloodstream the same way. If it does, then we know it will behave the same in patients. The brand-name drug already proved it works for treating the condition. The generic just needs to prove it gets there the same way.
For most pills - the kind you swallow - this works perfectly. But not all drugs are made the same. Inhalers, eye drops, skin creams? Those are trickier. You can’t measure how much of an asthma inhaler ends up in your lungs the same way you measure a pill in your blood. For those, regulators use different methods: clinical outcomes, lung function tests, or even skin absorption rates. The goal is the same: prove the effect is identical.
Why This Saves Billions - And Why It Matters
Brand-name drugs cost tens of thousands of dollars to develop. Clinical trials? They can take over a decade. The FDA requires thousands of patients in those trials. Generic manufacturers don’t repeat any of that. They don’t need to prove the drug works. They only need to prove it behaves the same in the body.
This is why generics cost 80% less on average. In 2020 alone, generic drugs saved the U.S. healthcare system $313 billion. That’s not a typo. That’s real money. And it’s not just about cost. It’s about access. If a drug costs $500 a month, many people skip doses or don’t fill the prescription. If it costs $5? They take it. Every day.
Over 90% of all prescriptions in the U.S. are filled with generics. And they’re not just common - they’re trusted. A 2022 Consumer Reports survey of 1,200 people found that 87% saw no difference between generic and brand versions. Nine percent even said the generic worked better. Only 4% felt it was less effective.
What Bioequivalence Testing Doesn’t Prove
It doesn’t prove the generic has the same inactive ingredients. That’s okay. Fillers, dyes, and binders don’t affect how the medicine works. But they can cause rare side effects - like a rash from a dye, or stomach upset from a different coating. That’s not a failure of bioequivalence. It’s just a difference in non-medical parts.
It also doesn’t guarantee identical performance in every single person. Some people metabolize drugs faster. Some have liver conditions. Some take other meds that interfere. Bioequivalence testing looks at averages across a group. It doesn’t predict every individual’s reaction. But it ensures that, for the vast majority, the effect is the same.
And there’s one more thing: it doesn’t apply to every drug. Drugs with a narrow therapeutic index - where the difference between a helpful dose and a harmful one is tiny - get extra scrutiny. For these, like warfarin or lithium, regulators sometimes require tighter bioequivalence ranges or even post-market studies. But even then, the standard remains the same: prove it behaves the same in the body.
Global Standards - And Why They’re Aligned
The U.S. isn’t alone. The European Medicines Agency (EMA), Health Canada, Japan’s PMDA, and others all use the same 80%-125% rule. The International Council for Harmonisation (ICH) made sure of that. Why? Because science doesn’t care about borders. If a drug works the same way in one country, it should work the same way everywhere.
And it’s working. In 2022, the global generic drug market was worth $438 billion. By 2030, it’s expected to hit $781 billion. That growth isn’t accidental. It’s built on decades of proven science.

Myths vs. Reality
People still believe generics are weaker. That they take longer to kick in. That they’re made in shabby factories.
Here’s the truth:
- Myth: Generics are made in lower-quality facilities. Reality: The FDA inspects over 1,200 generic manufacturing sites every year - same as brand-name plants. No exceptions.
- Myth: Generics aren’t as potent. Reality: They must deliver the exact same amount of active ingredient. Within 1%.
- Myth: If it looks different, it’s different. Reality: Color, shape, and size are changed on purpose - so generics can’t be confused with brands. The active ingredient? Identical.
One study found that 32% of patients still think generics are less effective. But that’s not science. That’s perception. And perception changes when people see results.
What’s Next? More Sophisticated Testing
The FDA is now using computer models to predict how a drug behaves - not just in 30 people, but in thousands. These models, called PBPK (physiologically based pharmacokinetic), simulate how age, weight, liver function, and other factors affect absorption. This isn’t replacing bioequivalence studies. It’s helping them. For complex drugs - like long-acting injectables or skin patches - these models can reduce the need for large human trials.
And it’s working. In 2022, 95% of generic drug applications were reviewed on time. Approval times are faster. Standards are tighter. And the number of generic drugs approved keeps rising.
More than 20,000 generic products are on the market. Over 14,000 different versions of 4,000 brand-name drugs. All tested. All approved. All proven to work the same.
Does bioequivalence testing prove a generic drug is as safe as the brand-name version?
Yes - but indirectly. Bioequivalence testing confirms that the generic delivers the same amount of active ingredient at the same rate as the brand. Since the brand drug’s safety profile was already established through large-scale clinical trials, the generic inherits that safety data. The FDA requires that generic manufacturers follow the same strict manufacturing standards (GMP) as brand-name companies. Any differences in inactive ingredients are monitored for potential side effects, but the active ingredient - the part that affects your health - is identical.
Are there any drugs where bioequivalence testing isn’t enough?
Yes. For drugs with a narrow therapeutic index - like warfarin, digoxin, or cyclosporine - regulators apply stricter bioequivalence criteria, sometimes narrowing the acceptable range to 90%-111%. For topical creams, inhalers, and eye drops, where the drug acts locally rather than systemically, bioequivalence is harder to measure through blood tests. In those cases, the FDA requires clinical endpoint studies - like measuring lung function for inhalers or skin absorption for creams - to prove the effect is the same.
Why do some people say generics don’t work as well for them?
Most often, it’s not because the drug is less effective. It’s because the inactive ingredients - like fillers, dyes, or coatings - are different. Some people are sensitive to these, leading to mild side effects like stomach upset or a rash. Switching back to the brand or trying another generic brand can solve the issue. Rarely, a person’s body may process the drug differently due to genetics or other health conditions. But these cases are uncommon. In large surveys, fewer than 5% of users report noticeable differences.
How long does it take to approve a generic drug?
The full approval process for a generic drug typically takes 10 to 12 months. Of that, about 6 to 8 months are spent on the bioequivalence study itself - designing it, running it, analyzing the data, and submitting it. The FDA reviews the application and inspects the manufacturing facility. Under the Generic Drug User Fee Amendments (GDUFA), 95% of applications are reviewed on time. This speed is possible because the generic doesn’t need to repeat the original safety and efficacy trials.
Can a generic drug be approved without any human testing?
Rarely, but yes - under specific conditions. For some simple, well-understood drugs, the FDA may accept in vitro data alone. This means testing how the drug dissolves in a lab setting (dissolution profile) and showing it matches the brand exactly. If the drug is immediate-release, has a wide therapeutic index, and has a well-established dissolution method, human bioequivalence studies may be waived. But this applies to only a small fraction of generics - most still require the standard 24-36 volunteer study.

Write a comment
Your email address will not be published.
Recent Posts
-
 How to Buy Cheap Generic Lamictal Online: 2026 Price Guide April 30, 2026
How to Buy Cheap Generic Lamictal Online: 2026 Price Guide April 30, 2026 -
 Monitoring Your INR: Understanding Blood Thinner Levels and Targets January 27, 2026
Monitoring Your INR: Understanding Blood Thinner Levels and Targets January 27, 2026 -
 How Cultural Beliefs Influence the Decision for Vaginal Surgery September 26, 2025
How Cultural Beliefs Influence the Decision for Vaginal Surgery September 26, 2025 -
 How to Use Price Transparency Tools to Compare Drug Costs December 9, 2025
How to Use Price Transparency Tools to Compare Drug Costs December 9, 2025

11 Comments
It's wild how much fear is built around something so thoroughly proven. We trust generics with our lives every day, yet the stigma lingers like an old myth.
Oh sweet mercy, another person who thinks color = efficacy? Honey, if your pill looks like a rainbow, it's not because they cut corners - it's because they're legally forbidden from copying the brand's look.
Also, 87% saw no difference? That's not opinion. That's data. And data doesn't lie.
Let me tell you something they don’t want you to know - the FDA doesn’t test generics themselves. They approve based on what the company submits. And guess who pays for those studies? The generic manufacturers.
So who’s really running the show? Big Pharma’s shadow arm. They’re not competitors - they’re subsidiaries in disguise.
And don’t even get me started on the 80-125% range. That’s a 45% swing. If your blood pressure med fluctuates that much, you’re playing Russian roulette with your heart.
You’re not alone if you’ve had a bad experience - but that’s usually about fillers, not the medicine. Try a different generic brand. Often, it’s just a matter of finding the right one.
And yes - $5 vs $500? That’s not a savings. That’s a lifeline.
One thing people miss: bioequivalence doesn’t mean identical. It means functionally equivalent. Like two different engines that get you from A to B at the same speed and fuel use.
One might have a louder exhaust. One might need a slightly different oil. But they both work.
And that’s all we need.
90% of prescriptions are generics??
That’s not just science - that’s a revolution.
And I’m here for it. 🙌
My grandma takes 7 meds. All generics. All working. All costing less than her coffee.
Stop acting like this is magic. It’s just smart policy.
And yet, the system is rigged. You see, the 80-125% window? It’s not based on clinical outcomes - it’s based on statistical convenience. The FDA adopted it in 1981, because it was easy to measure. But what if someone metabolizes drugs 300% faster? What if their gut pH is off? What if their liver enzyme profile is a outlier? You’re not testing for them. You’re testing for the average. And the average doesn’t care about you. You’re a data point. A footnote. A statistical artifact. And that’s terrifying.
Stop overthinking it. The math works. The studies are solid. The savings are real. If you’re not dead from it, it’s working.
So let me get this straight - you’re telling me a pill that costs $5 is just as good as one that costs $500 because some math says so?
What about the placebo effect?
What about the psychological comfort of paying more?
What if your brain just needs to believe it’s expensive to work?
Are we really that fragile?
And why do all generics look like they were made in a cereal box?
Bioequivalence is a pharmacokinetic benchmark, not a therapeutic equivalence metric. The 80-125% CI for AUC and Cmax is derived from log-normal distribution models under fasted conditions. However, in real-world scenarios, food effects, CYP450 polymorphisms, and gut motility variations introduce significant inter-individual variability. Hence, while statistically valid, population-level bioequivalence does not guarantee individual therapeutic parity - particularly in polypharmacy cohorts.
i just took my generic blood pressure med and my heart felt weird like?? idk if its the pill or if i ate too much tacos last night or if the moon is in the 7th house?? idk man. i just know i used to feel fine on the brand and now im like… maybe i should switch back??